Case Report: Upper and Lower All-on-X with Zirconia FP1 Restoration


Patient Presentation
She was in her thirties—bright, articulate, and outwardly confident. But like many patients in similar situations, there was a quiet, persistent weight she carried. Years of deferred care, dental anxiety, and life’s competing priorities had gradually led to a state of dental neglect. What began as occasional discomfort and missed cleanings slowly progressed to chronic infections, broken teeth, and an inability to smile without self-consciousness.
From a social perspective, poor oral health had begun to shape her daily life in subtle but meaningful ways. She found herself covering her mouth when she laughed, avoiding close conversations, and hesitating in professional settings where confidence and appearance mattered. Smiling—something so natural and human—had become guarded.
From a medical standpoint, the consequences were more serious. Chronic periodontal disease and untreated decay had created a constant inflammatory burden. She experienced intermittent pain, difficulty chewing, and recurrent infections. Beyond the mouth, we know that untreated oral disease is associated with systemic concerns like cardiovascular health, metabolic conditions, and overall inflammatory load. What was happening locally was not isolated.
At some point, the tipping point came, not from pain alone, but from a decision. She chose to move forward. To leave the past behind and invest in her health, function, and confidence.


Clinical Reality: Terminal Dentition
Upon comprehensive evaluation, it became clear that most of her remaining dentition was in a state of advanced breakdown. Extensive decay, structural compromise, and severe periodontal involvement rendered the teeth non-restorable. While this can be a difficult realization for patients, it also opens the door to definitive, long-term solutions.
We discussed all options for managing terminal dentition:
The AO4 Concept and Its Role
Like many patients today, she had done her research. A quick search for implant solutions often leads to the widely promoted All-on-4 (AO4) treatment concept.
AO4 is an excellent solution in many cases, particularly:
The prosthesis in AO4 is typically an FP3, meaning it replaces not only the teeth but also a portion of the missing gum and bone structure. While highly effective, it often requires a bulkier prosthetic design to compensate for lost tissue.
When FP1 Becomes the Superior Choice
In her case, however, the clinical presentation told a different story.
She exhibited:
These are precisely the scenarios where an FP1 prosthesis should be strongly considered. An FP1 restoration is designed to replicate the natural tooth emerging from the gum–without replacing lost soft tissue. The result is:
However, this approach comes with a critical caveat: It is significantly more technique-sensitive.
Why?
Because unlike AO4, where implants are placed “where bone is available” and the prosthesis compensates, FP1 requires:
There is far less room for error. The implants must be placed exactly where the final teeth need to be.
A Personalized Approach, Not Cookie Cutter
The patient was intentional in her search. She wasn’t looking for a one-size-fits-all solution. She wanted a team that would listen, evaluate her unique anatomy, and offer a treatment plan tailored specifically to her.
That’s exactly what we did.
After thorough evaluation and discussion, we determined that an AOX treatment protocol utilizing six implants per arch—designed to support a full-arch FP1 prosthesis—would provide the optimal balance of:
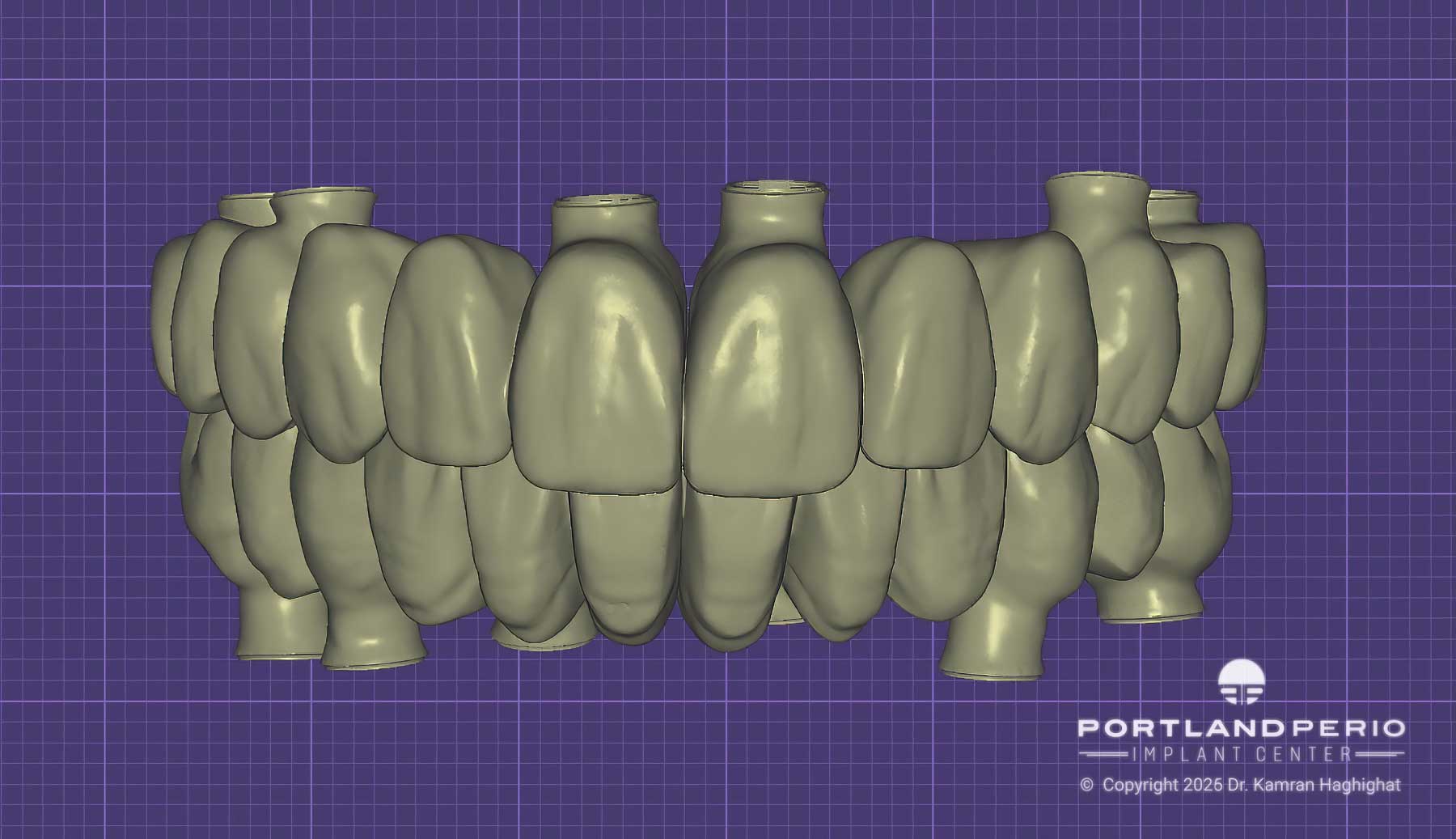



CAD CAM design
Digital Precision, In-House Execution
At our center, cases of this complexity are never approached generically.
Every step is guided by a fully digital workflow, including:
All design and fabrication processes are performed in-house, allowing us to:


Temporary Prosthesis designed and 3D printed in-house
Importantly, all provisional (temporary) prostheses are designed digitally and 3D printed in-house, ensuring rapid turnaround, precise fit, and the ability to refine and adjust designs efficiently throughout treatment.
The Importance of Temporization
One of the most critical—and often overlooked—aspects of full-arch rehabilitation is the transitional phase.
Throughout her treatment, she was provided with multiple provisional (temporary) restorations. These are not just placeholders—they are essential tools that allow us to:
This iterative process ensures that by the time we reach the final prosthesis, every detail has been tested, refined, and optimized.
Advanced Impression Technology
For the final restorative phase, we utilized photogrammetry technology—a highly accurate method of capturing implant positions digitally with micron-level precision.




Photogrammetry

Photogrammetry
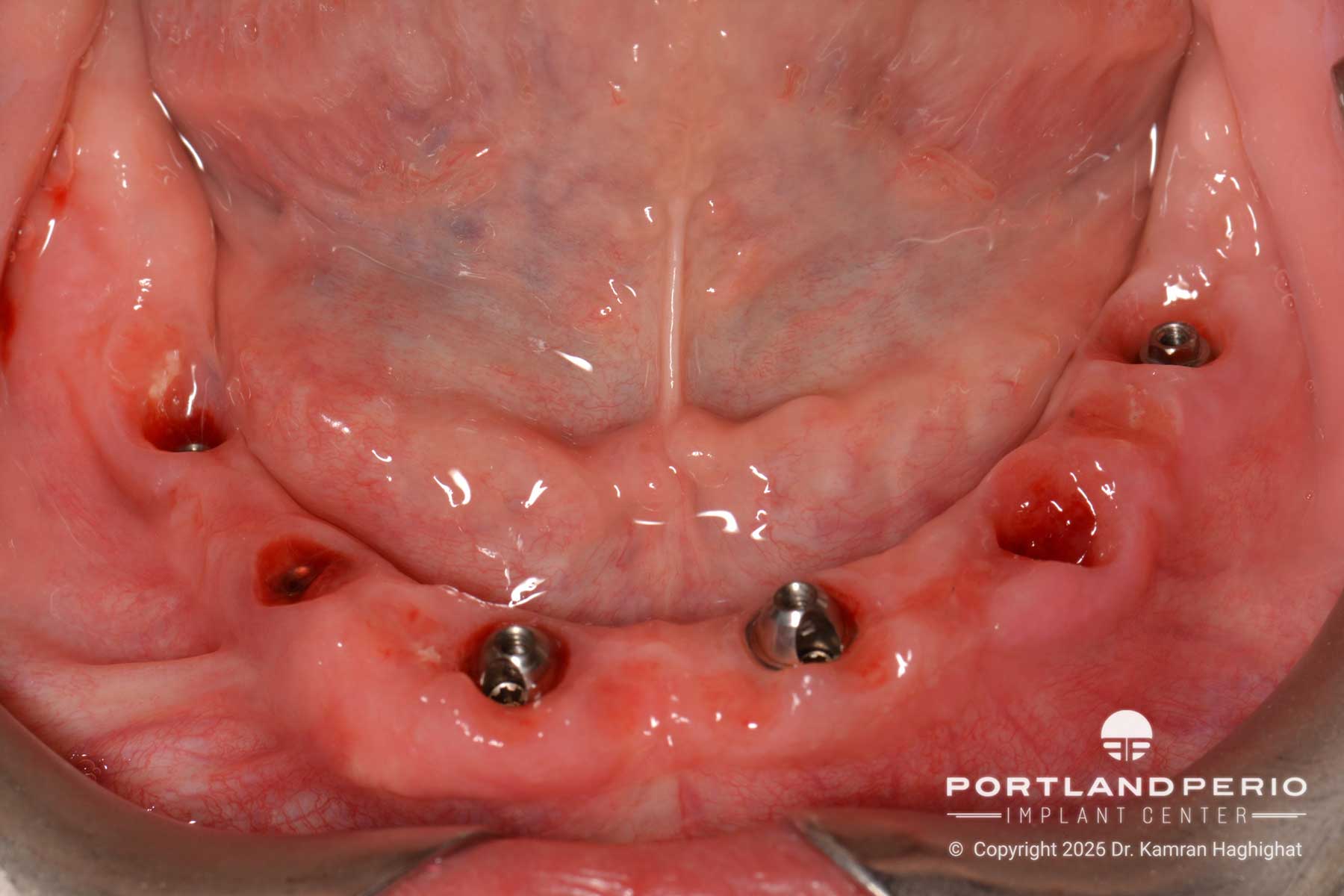
Tissue Sculpting
This eliminates many of the distortions associated with conventional or even standard digital impressions in full-arch cases, ensuring a passive, precise fit of the final prosthesis.
The Final Outcome
Her definitive restoration was fabricated from monolithic zirconia, selected for its:

Final Upper Zirconia Prosthesis

Final Bridges

Final Lower Zirconia Prosthesis

Final Upper Bridge
The result is a prosthesis that emerges naturally from the gingiva, closely mimicking the appearance of natural teeth—rather than sitting on top of the tissue, as is often necessary with bulkier hybrid designs.
The transformation was not just physical.
She smiles freely now. Speaks confidently. Eats without hesitation. The burden she carried for years—both visible and invisible—is gone.
This is more than a dental reconstruction.
It’s a restoration of health, identity, and confidence—built on thoughtful diagnosis, precise execution, and a commitment to treating each patient as an individual, not a template.

